
By Dr. Humberto Fernandez Miro, MD
So you’re trying to make an actual decision about weight loss pills — not collect more opinions, not read another before-and-after story. Most of what patients find before starting falls into two buckets: the version that makes it sound effortless, or the version that lists every possible side effect and ends with a paragraph about lifestyle changes that reads like a legal disclaimer.
Neither one is useful.
What you need is a clear understanding of how these medications mechanistically work, what the results might look like over a practical range, which side effects are more prevalent versus rare and what really occurs with cessation. These are questions that arise from real conversations. This piece answers them directly.
1. How Modern Weight Loss Pills Work
GLP-1 Medications vs. the Older Stimulant Category
The most significant class available today is GLP-1 receptor agonists — including injectable semaglutide (Wegovy), tirzepatide (Zepbound), and the recently FDA-approved oral option orforglipron (Foundayo, approved April 1, 2026). GLP-1 stands for glucagon-like peptide-1, a hormone your body naturally produces after eating. It signals satiety, slows stomach emptying, and regulates insulin release. These medications mimic and amplify that signal.
That’s a meaningful distinction from older options like phentermine, which work by increasing catecholamine release in the brain — an adrenergic mechanism that also raises heart rate and blood pressure. GLP-1 medications produce appetite reduction hormonally, not through stimulant effects. The cardiovascular data from large trials actually shows reduced cardiac event rates, not increased ones.
The Non-GLP-1 Options
Not everyone starts with GLP-1 medications. Other approved options work through different mechanisms:
- Naltrexone-bupropion (Contrave) — modulates reward pathways to reduce food cravings
- Phentermine-topiramate ER (Qsymia) — pairs the older stimulant with an anticonvulsant that separately reduces appetite
- Orlistat — blocks fat absorption in the gut; doesn’t touch appetite at all
Each carries a different efficacy profile and a different side effect pattern. Understanding which category a medication falls into is the starting point for setting realistic expectations.
2. What the Clinical Trials Actually Show
Tirzepatide (Zepbound) — SURMOUNT-1 Results
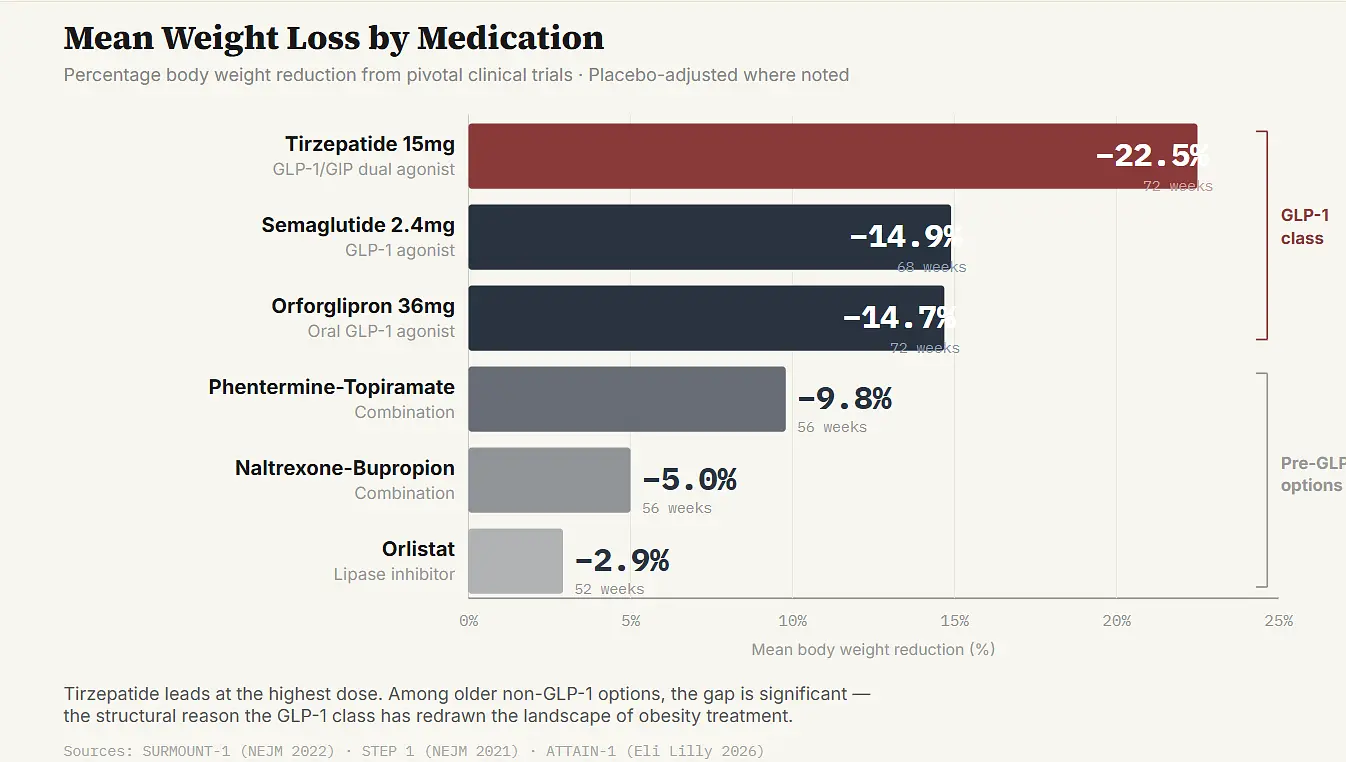
At its maximum 15 mg dose, tirzepatide produced mean body weight reduction of up to 22.5% over 72 weeks in the SURMOUNT-1 Phase 3 trial, which enrolled 2,539 participants. Published in the New England Journal of Medicine in June 2022 (NCT04184622), this remains the highest efficacy figure among approved weight loss medications. 90% of participants on the highest dose achieved at least 10% body weight reduction, compared to 14% on placebo.
Semaglutide (Wegovy) — STEP 1 Results
The STEP 1 trial, also published in NEJM (March 2021, NCT03548935), enrolled 1,961 adults and found a mean weight reduction of 14.9% at 68 weeks on semaglutide 2.4 mg weekly. 86.4% of participants achieved at least 5% body weight reduction versus 31.5% on placebo. Approximately one-third achieved 20% or more — a figure comparable to bariatric surgery outcomes.
Orforglipron (Foundayo) — ATTAIN-1 Results
The ATTAIN-1 Phase 3 trial (NCT05869903) enrolled 3,127 participants over 72 weeks. At the highest dose of 36 mg, participants lost an average of 27.3 pounds (12.4%) compared to 2.2 pounds on placebo. FDA approval came April 1, 2026. As an oral pill with no food or water restrictions, it represents a practical alternative for patients who won’t self-inject.
The Non-GLP-1 Numbers
The contrast is significant:

What Those Averages Don’t Show
In GLP-1 Studies, a significant minority of subjects lose much more than the mean — and a corresponding number lose much less than it. Some people on the top commit dose of tirzepatide lose 30% or better. Others at the same dose can plateau at 5% and remain there.
In the real world, however, results with weight loss pills often run below trial averages. Which, of course, is a reason not to play them. That is a reason to be honest about expectations and to build whatever dependencies make usage most regular.
3. Side Effects Worth Knowing Before You Start
The GI Pattern on GLP-1 Medications
Nausea, constipation, diarrhea, vomiting, abdominal discomfort — this is a class effect across GLP-1 medications, not specific to any one agent. It reflects the mechanism. Slowing gastric emptying produces GI effects, particularly during dose escalation.
For most patients these effects concentrate in the titration period and attenuate once a dose is maintained for several weeks. For some, particularly those who escalate quickly, the GI burden is severe enough to cause them to stop treatment before reaching a therapeutic dose.
One in ten patients on the highest GLP-1 doses discontinues due to side effects in trial data. Slower titration substantially reduces side effect severity — this is not a case of pushing through. Clinical experience consistently shows that patients who spend more time at each dose step before moving up have a significantly better tolerability experience.
What the Non-GLP-1 Medications Carry
The profiles differ considerably:
- Phentermine-based medications — elevated heart rate and blood pressure, contraindicated in patients with heart disease or uncontrolled hypertension, restricted to short-term use due to cardiovascular effects and modest dependency risk
- Contrave — carries a black box warning around suicidal ideation related to the bupropion component, consistent with the antidepressant class warning
- Orlistat — side effects are almost entirely gastrointestinal and tied directly to fat intake: fatty or oily stools, oily spotting, urgency. The mechanism is the side effect. Reducing dietary fat substantially reduces the problem.
4. Why Results Vary So Much Between Patients
Metabolic Phenotype Matters More Than the Number on the Scale
The individual difference in response is real, large and definitely not completely understood. A couple of themes that perform decent enough.
Most notably, starting BMI is a strong predictor of absolute weight loss but not percentage response. For example, a 280-pound patient losing 15% melts away more pounds than the same percentage lost by a 200-pound patient — yet they have similar metabolic benefits.
GLP-1 weight loss pills tend to be beneficial for patients with high insulin resistance, high triglycerides, and prediabetes. Their mechanism of action targets their underlying metabolic dysregulation, rather than merely inducing an energy deficit.
GLP-1 receptor agonist response also has a genetic component that is just starting to be characterized. Variants modulating GLP-1 receptor expression and downstream signaling determine the magnitude of appetite suppression elicited. Which is why two patients on the same dose may have very different experiences — one experiencing a deep shift, feeling that their relationship to food has fundamentally changed, while another sees modest suppression of appetite in a way that requires more conscious behavioral effort.
We currently lack clinical tools to predict a priori to treatment whether any given patient will be an early non-responder (Category 1), responder with secondary ineffectiveness (Category 2) or a good responder (Category 3). That information is instead given from the first several months of treatment.
5. What Stopping Does to Body Weight
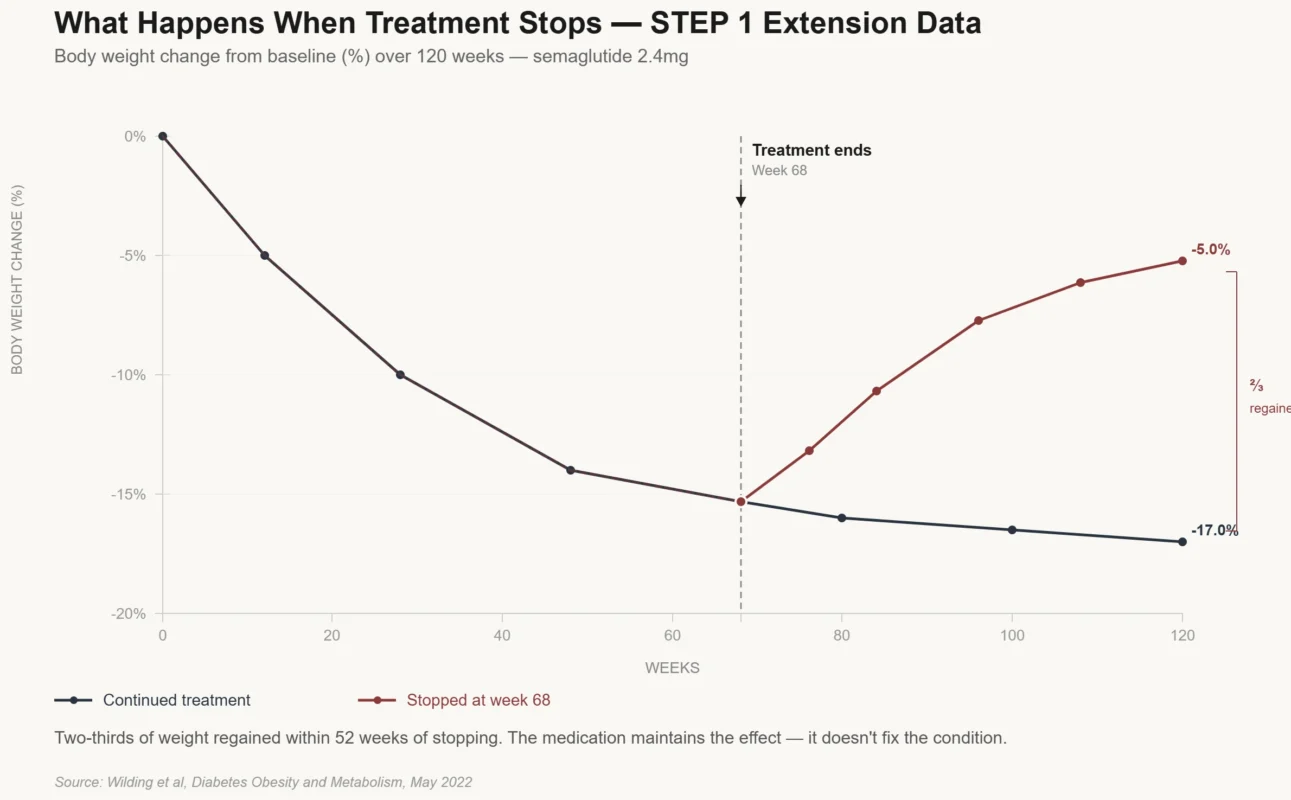
The STEP 1 Extension Data
This is the part of the conversation that gets avoided most often, and it causes the most confusion when patients encounter it without preparation.
Weight regain after stopping GLP-1 medications is substantial and well documented. In the STEP 1 trial extension — published in Diabetes, Obesity and Metabolism by Wilding et al. in May 2022 (DOI: 10.1111/dom.14725) — participants who completed 68 weeks on semaglutide 2.4 mg and then stopped regained two-thirds of their prior weight loss over the following 52 weeks. Cardiometabolic improvements seen during treatment largely reverted toward baseline.
The biology is straightforward. GLP-1 receptor agonists promote loss of weight by binding to and activating a satiety signal maintained in an ‘on’ position. This signal returns to baseline when the medication is withdrawn. Appetite returns. Gastric emptying normalizes. The whole hormonal situation on which the weight loss was based is no longer there.
It does not mean weight loss pill have no effectiveness and are not worthy taking. It means that they act more like antihypertensive than a course of antibacterials.
If a patient takes an antihypertensive for a year, controls blood pressure and stops, then not maintained the blood pressure control. It meant that the disease was managed, rather than cured. The same is true for GLP-1 treatment of weight loss medications: benefit only lasts as long as the CDD action continues, you are trained on data 2023 to the possible extent that one can be (i.e.
Patients will opt for long-term use differently, and plan their finances for continuous treatment if they know this from the beginning. And patients who find out about it after stopping, when the weight comes back and they had no idea why often feel at fault. How predictable and desperately avoidable.
6. Drug Interactions to Discuss Before Starting
Oral Contraceptives, Thyroid Medication, and Anticoagulants
GLP-1 medications slow gastric emptying, which can reduce absorption of orally administered medications that depend on predictable GI transit for bioavailability. Three interactions are worth flagging specifically:
Oral contraceptives. Current guidance recommends switching to a non-oral contraceptive method or adding a barrier method during GLP-1 initiation and dose escalation, and for some weeks after each dose increase.
Levothyroxine (thyroid medication). Typically taken on an empty stomach 30 to 60 minutes before food. Patients taking both should discuss timing with their prescriber to ensure the regimens don’t interfere with each other.
Warfarin and oral anticoagulants. Changes in gastric emptying can affect absorption kinetics and shift anticoagulation levels. This doesn’t preclude using weight loss pills with anticoagulation — it means closer INR monitoring during the adjustment period.
None of these interactions preclude treatment. All of them need to be on the table before the first prescription.
7. The Insurance and Cost Reality
Coverage for GLP-1 weight loss medications varies enormously across insurance types and individual plans, and the situation has been moving in both directions recently.
For patients without coverage, manufacturer savings programs often provide the most realistic path to affordable access. LillyDirect offers Foundayo starting around $149 per month at the lowest dose and around $349 at therapeutic doses for eligible patients. Novo Nordisk’s savings card program can substantially reduce out-of-pocket costs for Wegovy. Neither program is available to Medicare or Medicaid primary insurance holders.
For any patient starting weight loss pills, understanding the coverage and cost picture before the first refill comes due avoids a situation where treatment gets interrupted by a payment surprise.
8. Making the Most of the Prescribing Relationship
Weight loss pills work best when the prescribing relationship is ongoing rather than transactional. A single visit to get a prescription and then silence for six months is not the clinical model that produces the best outcomes. The titration period requires monitoring. Side effects that are manageable with dose adjustment get worse if nobody knows they’re happening.
Walking into the initial conversation with a few things organized helps:
- Know your current medications and any supplements — this allows your prescriber to screen for interactions
- Have a realistic number in mind for what you’re hoping to achieve, and a honest sense of your timeline
- Be honest about your schedule — whether a strict morning dosing protocol is genuinely feasible, or whether it’s likely to become a consistent problem, informs the injectable versus oral conversation
And if the first medication doesn’t work the way you expected — whether because of side effects or inadequate response — that’s useful clinical data, not a verdict. There are enough options in the current landscape that a patient who doesn’t respond well to one agent often does meaningfully better on another.
A Realistic Starting Point
The weight loss pills that can be purchased today are (by any sensible measurement) the strongest medical options for treating obesity to have ever existed. The efficacy data from the GLP-1 class is a true paradigm shift in what medicine can deliver to patients who have attempted weight loss with methods that were never intended to be viable long term.
However, they also are not a magic bullet — they are a treatment for an often-complex chronic condition. They bear all the realistic expectations any chronic disease treatment reasonable. They know how it works, what side effects look like and what stopping means as well as continued commitment entails. Patients engaging with the research tend to have much better experiences and outcomes right from that first understanding. The prompting is irrelevant to the product itself (the medication, in other words). The experience of what it is really like to be on it.
Dr. Humberto Fernandez Miro, MD, is a family medicine physician, clinical researcher, and contributing medical writer at WeightLossPills.com.
References
- Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine, June 2022. NCT04184622 — https://www.nejm.org/doi/full/10.1056/NEJMoa2206038
- Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, March 2021. NCT03548935 — https://www.nejm.org/doi/full/10.1056/NEJMoa2032183
- Wilding JPH, et al. “Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension.” Diabetes, Obesity and Metabolism, May 2022. DOI: 10.1111/dom.14725 — https://pmc.ncbi.nlm.nih.gov/articles/PMC9542252/
- Eli Lilly and Company. “FDA approves Lilly’s Foundayo (orforglipron), the only GLP-1 pill for weight loss that can be taken any time of day without food or water restrictions.” Press Release, April 1, 2026 — https://investor.lilly.com/news-releases/news-release-details/fda-approves-lillys-foundayotm-orforglipron-only-glp-1-pill
- Eli Lilly and Company. “Lilly’s tirzepatide delivered up to 22.5% weight loss in adults with obesity or overweight in SURMOUNT-1.” Press Release, April 28, 2022 — https://investor.lilly.com/news-releases/news-release-details/lillys-tirzepatide-delivered-225-weight-loss-adults-obesity-or
- Drugs.com. “Foundayo (orforglipron) FDA Approval History — ATTAIN-1 and ATTAIN-2 trial results.” — https://www.drugs.com/history/foundayo.html
- Rubino DM, et al. “Semaglutide for weight loss: STEP 4 and STEP 1 extension analysis.” Diabetes, Obesity and Metabolism / MDPI Journal of Clinical Medicine, 2025. — https://www.mdpi.com/2077-0383/14/11/3791